Physical Birth Trauma & the Brain-Injured Baby: What Should Mothers Know?
Share This
History of Childbirth Physical Trauma
For over a quarter of a millennia, doctors have recognized that physical or mechanical trauma at birth can endanger the fetus and damage or destroy fetal tissues.1 Prior to the Revolutionary War, one of the fathers of obstetrics, a Scottish doctor named William Smellie, had this to say: "In lingering labor, when the head of the child has been in the pelvis so that the bones ride over one another and the shape is prenaturally lengthened, the brain is frequently so much compressed that violent convulsions ensue before or soon after delivery to the danger and oft times the destruction of the child."2
Physical Birth Trauma Today
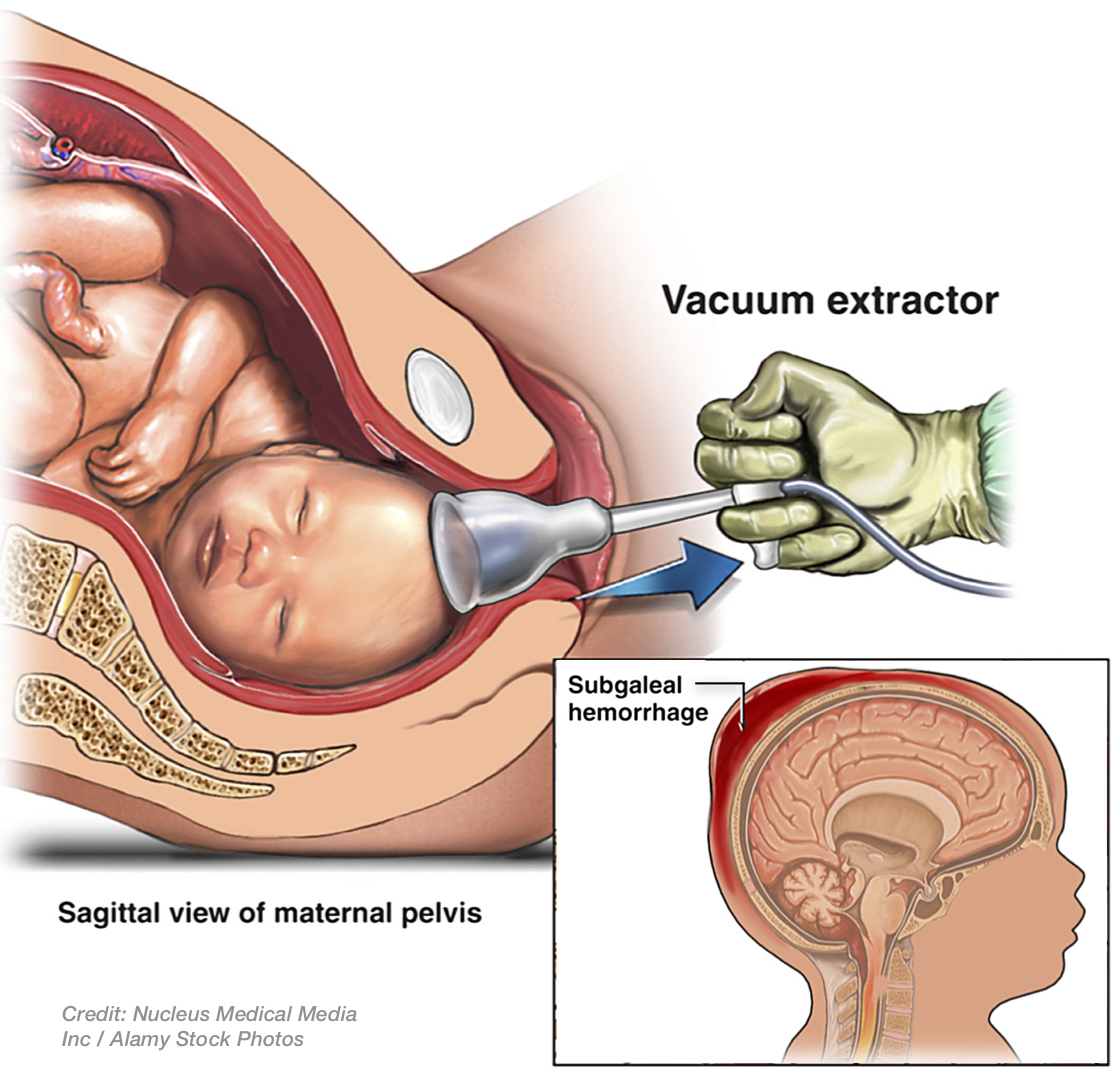
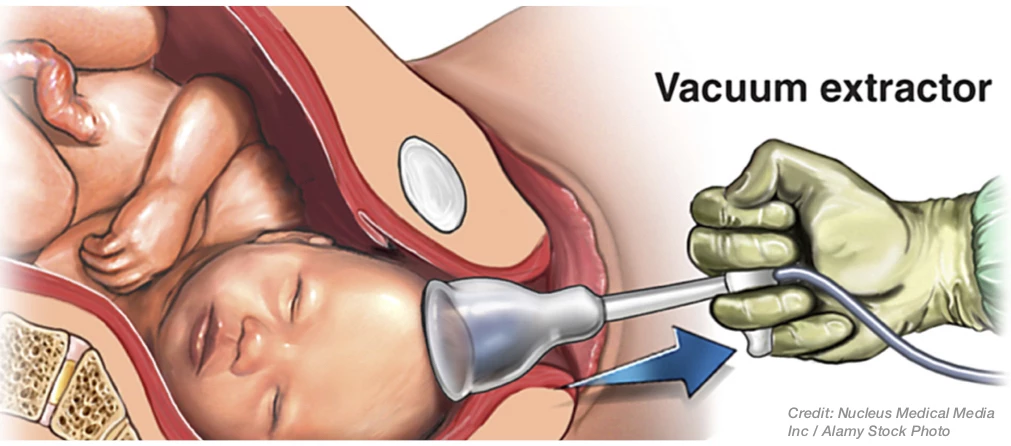
Despite centuries of advancements in medicine and technology, the fact is that head trauma to fetuses and babies still occurs too frequently during labor or delivery. In labor, when the baby's head descends (usually upside-down) before its body through the birth canal, there is a potential for physical damage to the fetal scalp, scalp layers, skull, lining inside the skull (dura), veins underneath the dura, and/or brain tissue. Of course most vaginal deliveries result in none of these injuries or, if they do, the injuries are normally minor from the head-compressive forces of labor. This includes compression against the mother's uterus or pelvic bone, such as with molding of the skull, and fluid or bloody fluid beneath the outer scalp layer (caput succedaneum) or just underneath (cephalohematoma) but outside the skull. Thankfully, these injuries normally resolve in the first few days of life. Rarely, however, these labor forces on the fetal head can be so strong that they can result in bleeding between the scalp layer and the skull bone (subgaleal hemorrhage); and, this type of injury is most commonly seen with use of instruments deliveries, e.g. vacuum extractors or forceps, to deliver the baby.3 Subgaleal hemorrhage can cause so much blood loss that a baby can develop shock and die.4 With excessive traction on the baby's head from use of forceps or a vacuum extractor, the skull can even be fractured, or bleeding can occur beneath the skull, which is known is epidural or subdural hemorrhage or hematoma. 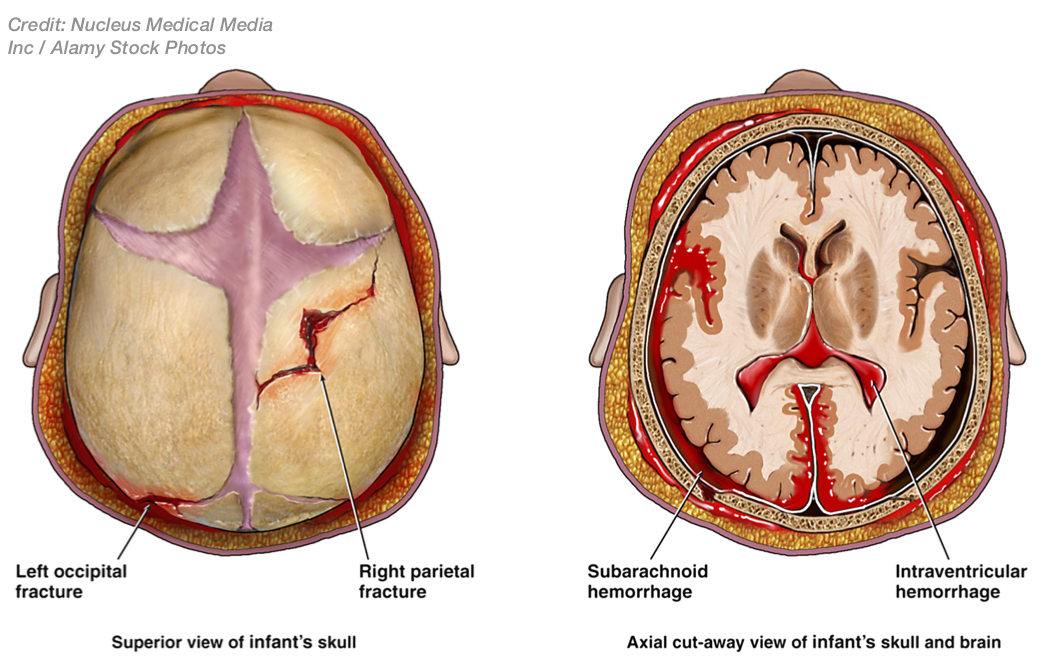 These types of injuries may result in permanent damage, depending on how quickly they are recognized and how properly they are treated. Moreover, these same instruments, when used improperly, can cause damage to vessels underneath the skull or in the brain or brain ventricles, resulting in intracranial bleeding, blood clots, stroke, and permanent injury. These injuries can also result in the following effects from the brain injury: shock from blood loss, hypotension (low blood pressure), apnea (periods of no breathing), bradycardia (slow heart rate), seizures, cardiopulmonary arrest and death. Surviving babies may have developmental delays, intellectual disabilities, cerebral palsy (involuntary motor dysfunction due to brain injury), and other serious neurological problems.5
These types of injuries may result in permanent damage, depending on how quickly they are recognized and how properly they are treated. Moreover, these same instruments, when used improperly, can cause damage to vessels underneath the skull or in the brain or brain ventricles, resulting in intracranial bleeding, blood clots, stroke, and permanent injury. These injuries can also result in the following effects from the brain injury: shock from blood loss, hypotension (low blood pressure), apnea (periods of no breathing), bradycardia (slow heart rate), seizures, cardiopulmonary arrest and death. Surviving babies may have developmental delays, intellectual disabilities, cerebral palsy (involuntary motor dysfunction due to brain injury), and other serious neurological problems.5
Vulnerability of the Fetus
To understand why a fetus or baby is at such risk with the improperly utilized vacuum extractor or forceps, two things must be appreciated. First, the baby's skull is very different from the adult skull because the connecting skull bones are not yet fused; this is why babies have fontanelles (soft spots) with just connective tissue between the skull bones, so-called "cranial sutures." So, the force from a vacuum extractor can displace and/or damage the bones, sutures, veins, and/or tissues, etc. Secondly, manufacturers of vacuum extractors warn doctors and midwives to be careful using these devices for precisely these reasons.6
The Current Warnings
In 1998, the FDA issued a public health advisory entitled, "Need for Caution When Using Vacuum Assisted Delivery Devices,"7 stating that a number of deaths and serious injuries had occurred from use of vacuum extractors that caused subgaleal hematomas and intracranial hemorrhages. Accordingly, in 2000 The American College of Obstetricians and Gynecologists (ACOG) recognized that "the incidence of intracranial hemorrhage is highest among infants delivered by caesarian following a failed vacuum or forceps delivery" and that "operative vaginal delivery should not be attempted when the probability of success is very low."8 Likewise, the FDA has given warnings and recommendations that care providers who use these devices should watch and be on the lookout for several hours after birth for signs or symptoms of damage from their use, including swelling, increased head size, pallor, tachypnea (fast breathing), tachycardia (fast heart rate), convulsions, etc.9
The Lawyer's Role
We are familiar with physical and mechanical birth trauma, and the injuries that may be afflicted on babies as a result. We work with highly qualified physicians and expert witnesses, in numerous fields, to model and/or link these forces to the child so injured in labor and/or delivery. And we have had significant past success in prosecuting these types of cases to substantial settlement.
Contact Us
If you are concerned that your child or a loved one's may have physical birth trauma due to events in labor or delivery, or due to events that occurred in a healthcare setting, you can email us at [email protected], or call us Toll-Free at 1-800-610-2546 for a free and confidential consultation.
Sources
- Kriewall, T, et al, Effects of Uterine Contractility on the Fetal Cranium, Ch. 7, A Short History of Obstetrics and Gynecology (1960).
- Id.
- Id.; Little, W., On the Influence of Abnormal Parturation, Difficult Labors, Premature Birth and Neonatorium, on the Mental and Physical Condition of the Child, Especially in Relation to Deformities, Trans. Obstet. Soc., Vol 3, p. 251 (London 1862), republished in Clin Orthop Relat Res., Vol. 46, pp. 7-15 (1966); Yates, P., Birth Trauma to the Vertebral Arteries, Arch Dis Child., p. 436 (1959); Clyne, D., Traumatic Versus Anoxic Damage to the Foetal Brain, Develop Med Child Neurol., Vol. 6, pp. 455-57 (1964); Kelly, J., Compression of the Fetal Brain, Am J Ostet Gynecol., Vol. 85, p. 687 (1963); Hanigan, WC, Morgan, AM, et al, Tentorial hemorrhage associated with vacuum extraction, J. Pediatr., Vol. 85, No. 4, pp. 534-39 (Apr. 1990); Govaert, P., et al, Traumatic Neonatal Intracranial Bleeding and Stroke, Arch Dis Child. Vol. 67, pp. 840-45 (1992); Sorbe, B., et al, Some Important Factors in the Molding of the Fetal Head During Vaginal Delivery‚ Photographic Study, Int J Gynaecol Obstet., Vol 21, pp. 205-11; Steinbrok, P., et al, Acute Subtotal Hematoma Associated with Cerebral Infarction in the Full Term Neonate, Pediatr Neurosurg., Vol. 23, p. 206 (1995).
- Shah, NA, Wusthoff, CJ, Intracranial Hemorrhage in the Neonate, Neon. Network, Vol. 35, No. 2, pp. 67-69 (March -Apr. 2016); Jensen, CB, Galbraith, SS, Iatrogenic and Traumatic Injuries, Ch. 8 (Clinical Gate), found at: http://clinicalgate.com/iatrogenic-and-traumatic-injuries/.
- Shah, n4, generally; Adiego, B, Martinez-Ten, P, et al, Fetal intracranial hemorrhage. Prenatal diagnosis and postnatal outcomes, J Matern-Fet & Neon Med. (Sep. 4, 2017); O'Leary, JA, Shoulder Dystocia and Birth Injury, Prevention and Treatment (1992).
- See, e.g., Kiwi-Complete Vacuum Delivery System with Palm Pump, Clinical Innovations, p. 11 (2014)("stating "[d]o not twist, torque or use excessive force."); Mityvac Reusable Silicone Vacuum Extraction Cup Instructions for Use, Cooper Surgical (Apr. 2018)(stating "[d]o not exceed recommended levels," and "abandon vacuum-assisted delivery if the vacuum cup disengages (pops off) three times," etc.); Operational Guidelines for use of The Mityvac Obstetrical Vacuum System (Mar. 1997)("Caution: Incorrect use of this device could possibly cause‚ fetal bruises, contusions, lacerations, fractures, intracranial hemorrhage, cephalohematoma, subdural hematoma, subgaleal hematoma, parenchymal hematoma, and retinal hemorrhage.").
- U.S. Food & Drug Administration (FDA) Center for Devices and Radiological Health, Public Health Advisory: Need for Caution when using vacuum assisted delivery devices (May 21, 1998).
- ACOG, Practice Bulletin No. 17, Operative Vaginal Delivery (June 2000).
- FDA Patient Safety News, Problems After Vacuum-Assisted Childbirth, (June 5, 2002).